


Note: This is not medical advice and is not equivalent to the doctor’s observation.
Condition-Specific Effectiveness of Therapy and Medication?
If trauma, insomnia, or ADHD are central problems, targeted approaches, trauma-focused therapy, CBT-I, or ADHD therapy with or without medication, improve outcomes. The goal isn’t either/or; it’s the right mix that fits your life and delivers measurable progress.
Struggling to Decide Between Therapy or Medication?
Short Answer of Medication Vs Therapy
Why “either-or” often Fails: What Causes Symptoms in the First Place
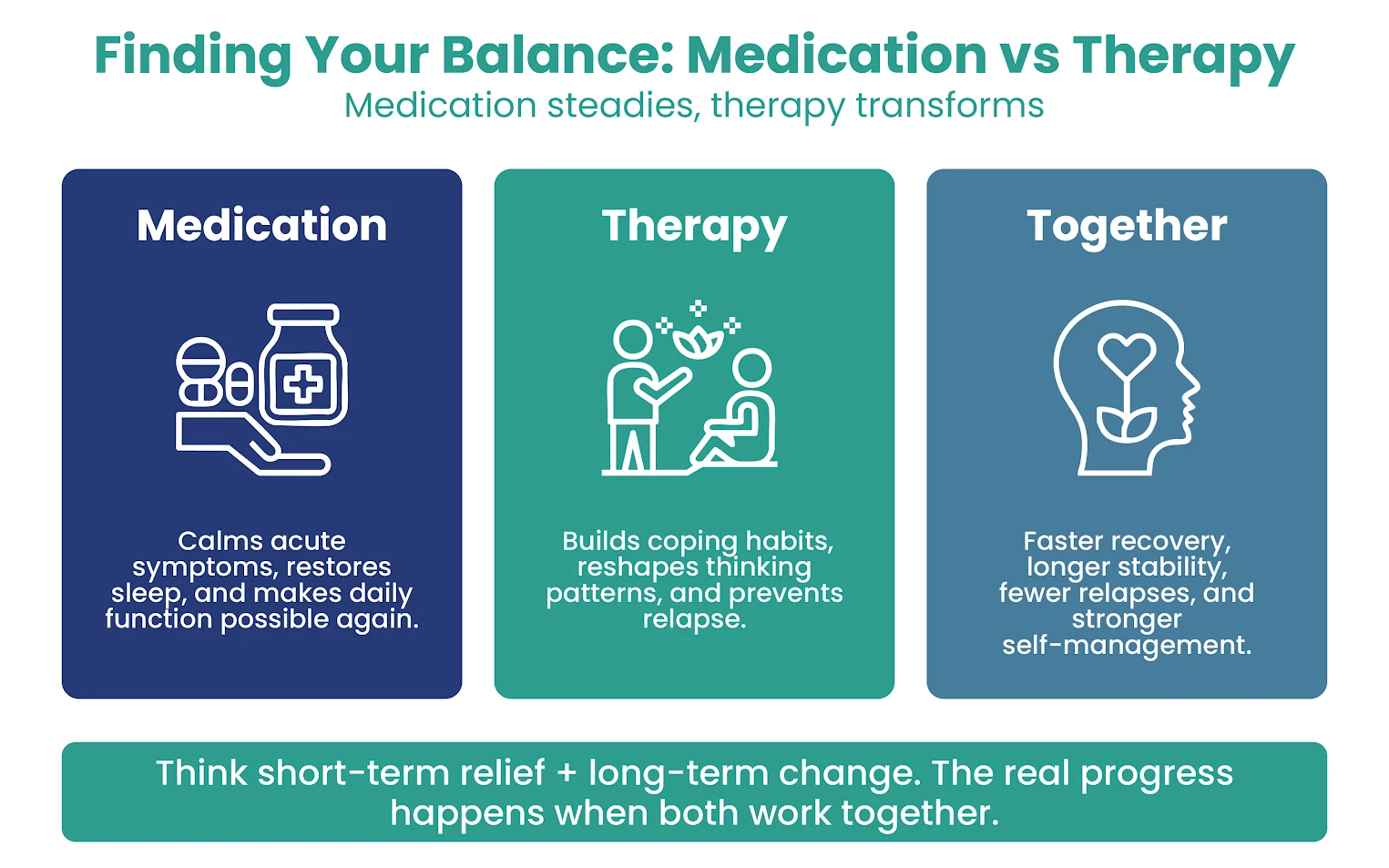
- Medication (SSRIs/SNRIs, mood stabilizers, antipsychotics, stimulants) can quickly blunt severe arousal or low mood.
- Mental health therapy (CBT, exposure, IPT, DBT, family work, CBT-I) retrains patterns that keep symptoms going, builds coping skills, and protects against relapse.
Expert Insights
Think of a broken leg: the medication stabilizes early; physical therapy (psychotherapy) restores function. Most people benefit when medical therapy and standard therapy are coordinated.
Condition-by-Condition: Key Causes, Symptoms, and What Works
Why and How of Depression and What Works
Common Drivers (causes)
Symptoms to Watch:
Best-Supported Treatment
What Works Best
Pro Tips for OCD, PTSD, bipolar, and psychosis
- OCD: ERP is essential; SSRIs help but don’t replace exposure. If meds only partially help, add ERP, don’t just change doses endlessly.
- PTSD: trauma-focused therapy (PE, CPT, EMDR) is first-line; SSRIs can reduce hyperarousal/sleep problems to let trauma work proceed.
- Bipolar disorder: mood stabilizer/atypical antipsychotic first; therapy adds relapse prevention, routine, and trigger plans.
- Psychosis: antipsychotic medication is foundational; CBT targets residual voices/paranoia and social withdrawal.
- Pro Tip: If you’ve done “talk therapy” without targeted methods (ERP, CPT, CBT-I), ask for method-specific treatment; technique matters.
Why and How of Anxiety Disorders and Treatment
Common drivers:
Symptoms:
Best-supported treatment:
Why and How of Obsessive Compulsive Disorder (OCD) Treatment
Common drivers:
Symptoms:
Obsessions (contamination, harm, checking) and compulsions (washing, repeating, reassurance).
Best-supported treatment:
Why and How of PTSD and Trauma-Related Conditions Treatment
Common drivers:
Symptoms:
Best-supported treatment:
Are You Feeling Stuck on Medication Alone?
Why and How of ADHD Treatment
Common drivers:
Symptoms:
Best-supported treatment:
Why and How of Bipolar Disorder Treatment
Common drivers:
Mood regulation circuitry with genetic loading; sleep disruption as a trigger.
Symptoms:
Best-supported treatment:
Therapy Helped, But You’re Still Not Yourself?
Sometimes the missing piece is biological. Our psychiatrists review whether medication support could unlock the next level of recovery.
Why and How of Schizophrenia and Psychotic Disorders Treatment
Common drivers:
Symptoms:
Best-supported treatment:
Why and How of Insomnia and Treatment Options
Common Drivers:
Symptoms:
Best-supported treatment:
Personality Disorders & Chronic Interpersonal Patterns
Common Drivers:
Symptoms:
Best-supported treatment:
What High-Quality Studies Say About Therapy vs Medication
- No single overall winner for depression: Direct comparisons show similar end-of-treatment symptom relief with psychotherapy vs antidepressants.
- Combination care is often best: Therapy + medication shows small-to-moderate added benefits for functioning and quality of life, and better relapse prevention in maintenance care than either alone.
- Acceptability matters: Patients drop out less from psychotherapy than from medication in many trials. Lower dropout aligns with better outcomes—use what you can stay with.
- Duration counts: Depression treatments >3 months are more likely to produce quality-of-life gains than very brief courses.
- Cost-effectiveness is equal over time: Over ~5 years, CBT and antidepressants are similarly cost-effective; offering both and honoring patient preference is sensible care.
- Symptom-level “matching” hasn’t cracked the code: Attempts to assign depression treatment based on individual symptom profiles did not reliably outperform standard selection. Personal factors (severity, trauma history, preference, prior response) still guide best.
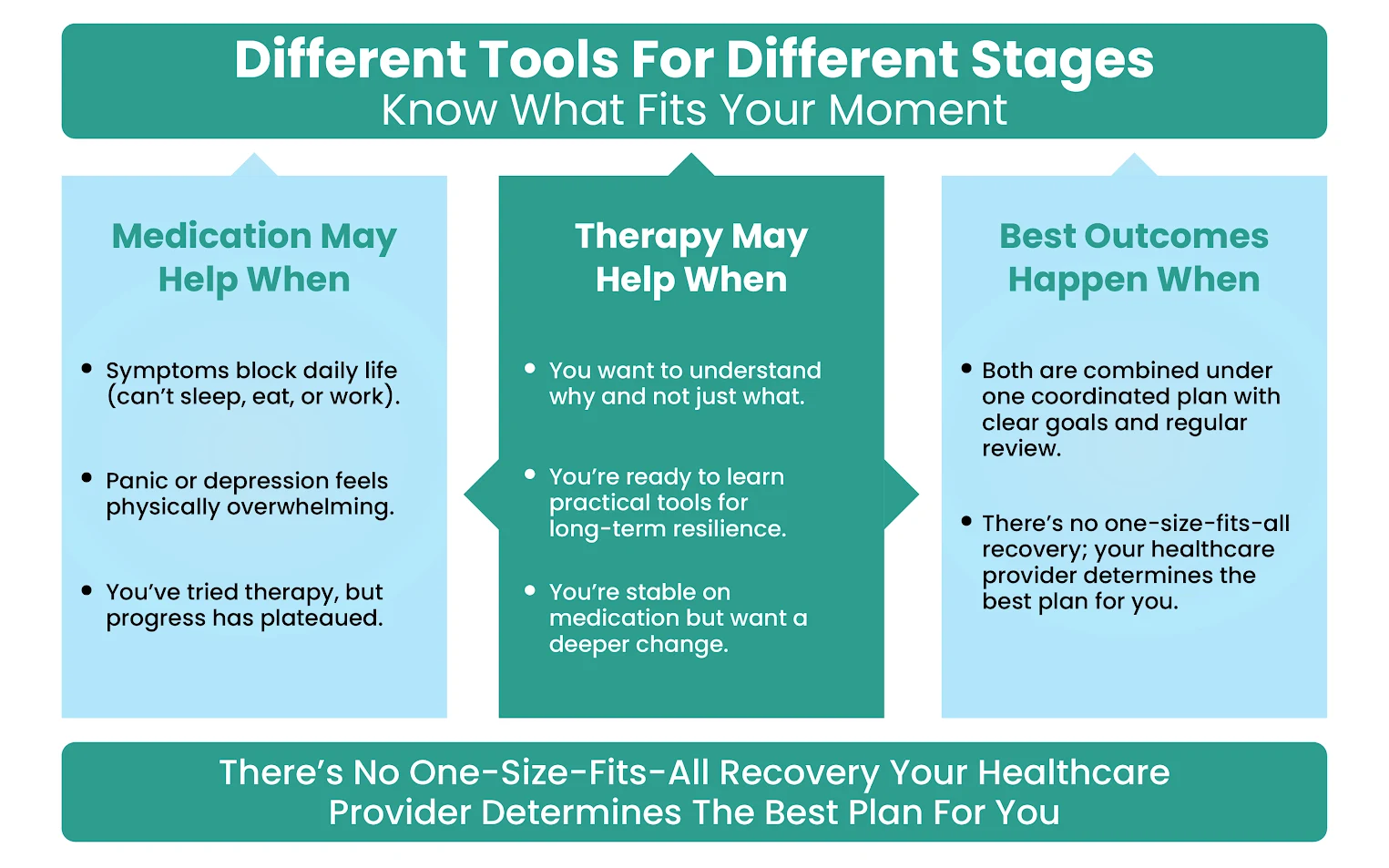
How to Choose (fast) without Guessing
Quick rule of thumb:
- Mild–moderate → start therapy (CBT/IPT); add meds if no clear gains by 4–6 weeks.
- Moderate–severe, crisis, or insomnia/appetite collapse → start medication + schedule therapy within 2 weeks.
- Combination wins when you need speed + durability (rapid symptom relief from medication; relapse prevention and skills from therapy).
- Pro Tip: Tell your clinician, “My priority is to stabilize sleep and panic now, then build long-term skills—can we plan meds + CBT and review at week 4?”
Safety, Side Effects, and Smart Medication Management
- Benzodiazepines (e.g., alprazolam, lorazepam, clonazepam) can be helpful in the short term, but long-term use risks tolerance, dependence, cognitive side effects, and dangerous interactions (especially with alcohol or opioids).
- Antidepressants/antipsychotics/mood stabilizers require dose optimization, side-effect monitoring, and periodic reassessment. If a regimen isn’t working, consider switching, augmenting, or leaning more on psychotherapy skills, and avoid stacking multiple meds without a clear benefit (polypharmacy).
- When meds aren’t enough: Robust data show that adding CBT/ERP to partial medication responders (OCD, anxiety, depression) improves outcomes.
Safety, side effects, and when to pivot
- Side effects window: many SSRI effects fade by week 2–3; if intolerable (e.g., severe agitation, rash, suicidal thoughts), call immediately.
- Benzodiazepines: short, targeted use only if prescribed; avoid daily long-term reliance—build CBT skills instead.
- Know the pivot points: no functional gains by week 6–8 → adjust dose/switch class or add the missing modality (therapy ↔ meds).
- Pro Tip: Bring a side-effect log (date, severity, duration, what helped). It speeds safe adjustments and prevents unnecessary switches.
Your Practical Decision Checklist of Therapy Vs Medication
Start with these questions:
- Severity/urgency: Are you in crisis or unable to function? If yes, consider pharmacologic therapy first for stabilization, then add therapy.
- Core maintenance loops: Are symptoms maintained by avoidance, reassurance, or catastrophic thinking? If yes, CBT/exposure should be central.
- History: What worked, or caused side effects, before? Repeat success; avoid prior pitfalls.
- Trauma history: Significant trauma often points to trauma-focused therapy as the lead.
- Access & cost: Which can you start now and sustain (sessions, copays, time)? “Over ~5 years, CBT and antidepressants are roughly equal in cost-effectiveness; preference and access should guide first-line choice.”
- Preference and adherence: You’re more likely to improve with a plan you believe in and will stick with.
- Children & teens: For ADHD under six, start with behavior therapy; for pediatric OCD, ERP + SSRI often outperforms either alone.
- Fast relief vs staying power: Medication can deliver quicker symptom control; therapy delivers skills that last. Many people choose both to cover now and later.
Get Matched with the Right Care Mix, Fast
Where AZZ Medical Associates Fits (In-Clinic & Telehealth)
- Therapy and medication under one roof: with acceptance of all incidences, coordinated psychiatry vs therapy planning so you’re not stuck relaying messages between offices.
- Same-day/weekend appointments when available; telehealth statewide in NJ plus 21+ local locations for in-person care.
- Evidence-based options: CBT, exposure therapy/ERP, IPT, DBT skills, CBT-I, medication management, and combination care for depression, anxiety disorders, OCD, PTSD, ADHD, bipolar disorder, psychotic disorders, insomnia, and more.
- We tailor treatment vs therapy sequencing to your symptoms, severity, and goals, and adjust quickly based on your response.
Bottom Line
- Causes: symptoms usually reflect both biology and learned patterns.
- Symptoms: define what you feel and how life is impacted to guide care.
- Treatment: for many conditions, therapy vs medication isn’t a contest; combining them often yields better functioning, quality of life, and relapse prevention.
FAQs
Is therapy or medication better for depression and anxiety?
Both are valid mental health treatments. For many, therapy and medication together are the most effective mental health treatment, improving quality of life and lowering relapse risk. If you prefer one, start there and add the other if progress stalls.
Do anxiety meds work, and for how long?
Yes. SSRIs/SNRIs can reduce anxiety; benzodiazepines work quickly but are best for short-term use due to risks. CBT/exposure often matches or exceeds meds and has more durable benefits.
Can I improve mental health without therapy?
Some do well with medication therapy alone. Yet therapy often addresses the underlying patterns (avoidance, catastrophic thinking), so many patients gain better long-term results by adding talk therapy.
Therapy vs antidepressants, how do I choose near me in NJ?
Book an evaluation at AZZ Medical Associates (in-person or telehealth near me). We’ll review severity, history, preferences, and access, then recommend therapy vs medication or a combination.
Can therapists recommend or give medication?
Therapists don’t prescribe. Our psychiatric medicine providers (MD/DO/NP/PA) manage pharmacological treatment while your therapist delivers psychotherapy, both coordinated.
Is this clinical advice?
Absolutely not. This is not clinical advice, although this article is written and peer-reviewed by medical experts and only includes the information from verified sources and citations. This is not medical advice and is not equivalent to the doctor’s (psychiatrists/psychologists) observation.




