What PRP Is & What It Isn’t
PRP Eligibility, Done Properly
How PRP Joint Injections May Help
- PRP delivers a higher-than-normal concentration of platelets to a target area.
- Platelets release growth factors that may support tissue repair, local cell activity, and the healing environment.
- In joint conditions such as osteoarthritis, early research suggests PRP may help by modulating inflammation inside the joint and improving the “joint environment,” which can translate into less pain and better movement for some patients.
What’s Inside PRP & Why Clinicians Use It
| PRP Component | Why it matters | What patients usually notice |
|---|---|---|
| Plasma (liquid portion) | Carries platelets and proteins to the target area | A “delivery medium,” not a painkiller |
| Platelets | Release growth factors involved in healing signals | Results tend to be gradual, not instant |
| Growth factors (examples: PDGF, TGF, VEGF, EGF, IGF) | Can signal cell activity, tissue recovery, and blood vessel support | Improvement often takes weeks |
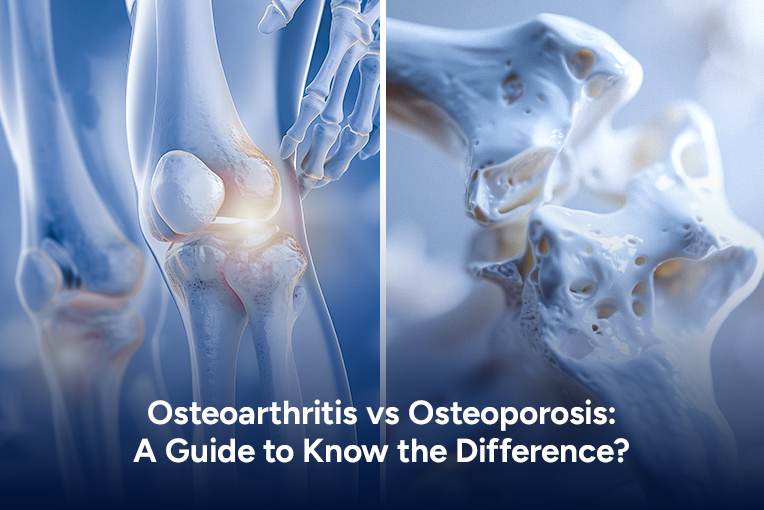
Where PRP is Commonly Used In Musculoskeletal Care
PRP for Knee Joint Pain (and osteoarthritis)
Elbow Pain: Tendons & “Joints at The Elbow.”
Ankle Pain: The Ankle Joint & Ligaments
Knee Pain, Better Decisions
What to Expect During a PRP Joint Injection Visit
- Assessment first
History, exam, and review of imaging when appropriate. Rheumatology focuses on confirming whether pain is mechanical (like osteoarthritis) or inflammatory (like rheumatoid arthritis, gout, or other autoimmune disease patterns). - Blood draw
The draw volume depends on the system used. Clinics commonly draw a small tube or several tubes. - Centrifuge processing
The blood is spun to concentrate the platelets into PRP. - Injection into the target area
A platelet-rich plasma joint injection may be delivered with ultrasound guidance, depending on the joint and the clinician’s preference. Ultrasound can improve accuracy, especially in smaller joints or deeper structures. - Aftercare
Mild soreness is common. Many protocols advise avoiding anti-inflammatory medications around the procedure window because they may interfere with the inflammatory-healing signaling PRP is trying to promote. Your clinician should give clear, personalized instructions.
Expert Insights
Rheumatology-first: PRP fails most often when diagnosis is wrong
A rheumatologist looks for the “why” behind pain, osteoarthritis wear, tendon overload, gout/pseudogout, autoimmune inflammation, or referred pain from hip/spine.
If the joint is truly inflamed (warmth, swelling, prolonged morning stiffness), treating inflammation and ruling out crystal disease may matter more than any injection.
At AZZ Medical Associates, use PRP only after the condition and target tissue are confirmed.
Precision-Guided PRP Injections
PRP Injection Vs Other Common Rheumatology Procedures
| Procedure | Main purpose | What it does |
|---|---|---|
| PRP joint injection | Support healing signals, reduce pain in select cases | Injects your own concentrated platelets into/around a joint |
| Corticosteroid injection | Fast inflammation relief | Can reduce swelling quickly, but doesn’t “regrow” tissue |
| Knee joint aspiration | Diagnose or relieve fluid buildup | Removes joint fluid; sometimes paired with other treatments |
| Physical therapy | Restore strength and mechanics | Improves movement patterns and reduces overload on joints |
When Results Show Up, & How Long They Last
Side Effects, Risks, & Who Should Avoid PRP
- Soreness, tenderness, & bruising at the injection site
- Occasionally, swelling or short-lived discomfort
Expert Insights
How to get more value from PRP: treat the joint like a rehab project
PRP isn’t a standalone fix. Outcomes improve when you pair it with:
(1) A progressive strengthening plan for surrounding muscles.
(2) Load management for 2–4 weeks (no “stress-test” workouts).
(3) Mechanics correction (gait, footwear, training errors).
Ask for a simple function metric (stairs, walking time, pain diary) so you measure progress, not just “how it feels today.”
AZZ Medical Associates can help structure this so PRP supports real-life function.
Table 3: Candidate Checklist for PRP for Joints
| Often a better fit | Often not a fit (or needs specialist clearance) |
| Early-to-moderate joint pain with a clear target | Active infection or fever |
| Tendon/ligament pain that hasn’t improved with basics | Platelet disorders / very low platelet count |
| Patients who want a non-steroid option | Sepsis, uncontrolled systemic illness |
| Those who can follow aftercare guidance | Certain cancers or major contraindications based on history |
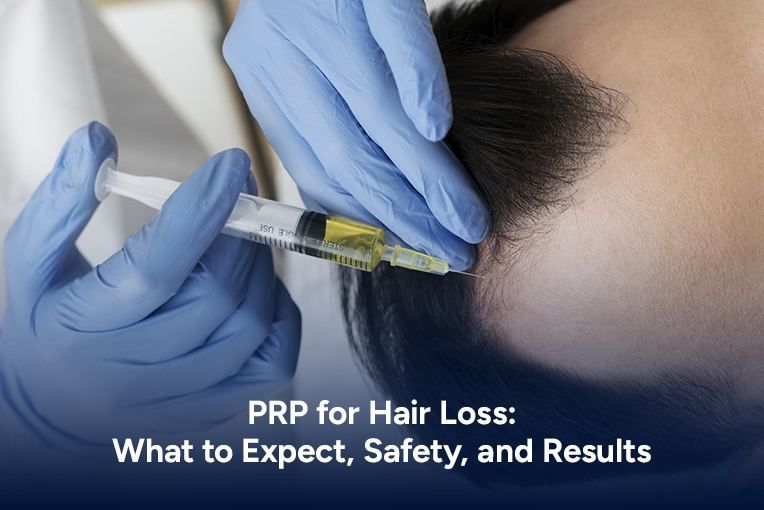
PRP Injection for Hair Loss & Joints: The Connection & the Difference
Quick table: A clinical Hair PRP Study Snapshot
| Study setup | Treatment pattern | What was observed |
| PRP on half scalp vs placebo on the other half | 3 sessions about 30 days apart | Hair count and density improved after treatment; a minority needed retreatment later |
Common Questions
Do PRP injections for joint pain work for everyone?
No. Some people improve meaningfully; others notice little change. Protocol differences, the exact diagnosis, and the severity of tissue damage all influence results.
What’s the best pain reliever for knee joint pain after PRP?
There isn’t one “best” option for everyone. Many clinicians prefer avoiding anti-inflammatory drugs around PRP because they may interfere with the intended healing response. Your rheumatology team can suggest safer short-term options based on your history.
Is PRP “joint rejuvenation therapy”?
That phrase is often used in marketing. PRP may support a healthier local environment and reduce pain in select cases, but it doesn’t reverse advanced arthritis or replace cartilage as a new joint would.
Next steps
Build a Joint Plan