Persistent Depressive Disorder vs. Major Depressive Disorder
- PDD (dysthymia): Low mood most days for ≥2 years in adults (≥1 year in youth) plus at least two associated symptoms (e.g., low energy, poor concentration, sleep or appetite change, low self-esteem, hopelessness). Remissions never exceed two months.
- MDD: A two-week episode with five or more symptoms (e.g., anhedonia, marked weight/sleep changes, psychomotor change, guilt, suicidal thoughts).
Do you know
Interestingly, both can co-occur. When an MDD episodes coincide with longstanding dysthymia, clinicians may call it “double depression.” Correct labeling affects treatment planning and insurance authorizations.
Symptoms of Persistent Depressive Disorder
Constant low mood, depleting energy, sleep or appetite change, poor concentration, indecision, low self-esteem, and persistent hopelessness define the pattern of PDD. People push through, try to use the power of decision (limited), then crash and feel demotivated and hopeless.
Core Symptoms of MDD
- Low energy, easy fatigability, slower task initiation
- Sleep disturbance (insomnia or hypersomnia)
- Appetite change (undereating or overeating)
- Low self-esteem; self-criticism; feeling “never enough”
- Poor concentration, indecision, missed deadlines
- Social pullback, less pleasure, chronic hopelessness

Persistent Depressive Disorder in Teenagers
PDD in Adults
Causes & Risk Factors of Persistent Depressive Disorder
- Neurobiology: Differences in neurotransmission (serotonin, norepinephrine) and stress-response systems
- Genetics/family history: Depression and dysthymia cluster in families
- Early adversity: Loss, trauma, chronic criticism, or unstable caregiving
- Chronic stress & medical illness: Pain, sleep disorders, thyroid issues, diabetes
- Temperament: Self-critical style, high dependence, persistent pessimism
- Epidemiology: Women are affected more often; onset commonly in youth/early adulthood
Diagnosis: DSM-5 & ICD-10
- Depressed or irritable mood most days for ≥2 years (adults) or ≥1 year (children/teens)
- While depressed, at least two: poor appetite/overeating; insomnia/hypersomnia; low energy/fatigue; low self-esteem; poor concentration/indecisiveness; hopelessness
- No symptom-free period longer than 2 months
- No manic/hypomanic episodes; not better explained by another disorder or substance/medical cause
Expert Insights
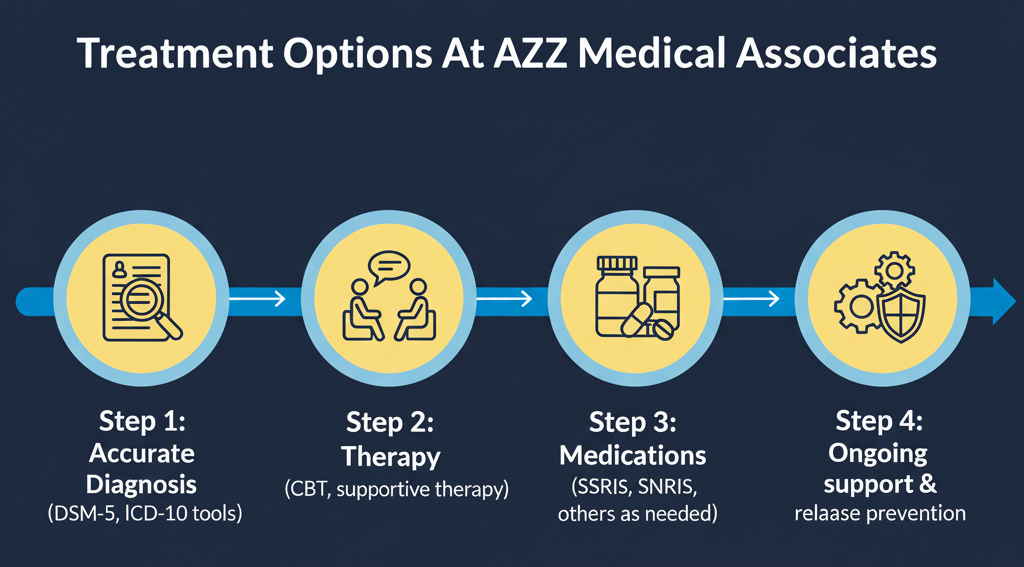
Treatment Options of AZZ Medical
- Cognitive Behavioral Therapy (CBT): It focuses on changing negative thoughts, beliefs, and rumination and replacing them with positive ones. Emphasizes behavioral activation, problem-solving, and relapse prevention. Delivered via in-clinic and via telehealth.
- Interpersonal Therapy (IPT): A person can also be affected by losses and social disruptions. IPT addresses these problems and works to maintain your mood.
- Medication: SSRIs/SNRIs are first-line (bupropion or mirtazapine), they may help the patient get back energy, better sleep, or appetite cycle. Augmentation can be considered if there is a partial response. Expect 4–6 weeks for early benefit.
- Lifestyle scaffolding: Regular sleep/wake times, movement most days, light exposure, reduced alcohol/cannabis, and structured social contact.
Get Care that Prioritize Your Time & Convenience
CBT Therapy for Persistent Depressive Disorder
- Behavioral activation: Rebuilds rewarding activity and momentum
- Thought work: Identifies automatic negativity (“I’m a failure”), tests evidence, and updates core beliefs
- Skills for stickiness: Planning tools, graded tasks, problem-solving, and relapse plans
- Sleep & rhythm: Stimulus control, wind-down routines, and social rhythm therapy for circadian stability
Medication Management
Medication supports brain systems that regulate mood and energy:
- First-line: SSRIs (e.g., sertraline, escitalopram) or SNRIs (e.g., venlafaxine, duloxetine)
- Alternatives/adjuncts: Bupropion (energy/focus), mirtazapine (sleep/appetite), buspirone augmentation in selected cases
- Follow-through: Continue meds several months after remission; taper only with clinician guidance
Self-Help & Day-to-Day Management
Small, repeatable changes matter:
- Consistent sleep window; morning light; limit late-night screens
- 20–30 minutes of movement most days (walks count)
- Scheduled “micro-rewards” to rebuild pleasure
- Reduce alcohol/cannabis; moderate caffeine
- Brief daily check-ins: mood, tasks, contact with one person
- Keep a relapse plan: early-warning signs, who to call, rapid steps
How to Manage Persistent Depressive Disorder Long-Term
- Therapy “booster” sessions after acute treatment
- Medication adherence and periodic review
- Calendarized routines (sleep, meals, movement, social time)
- Track stressors; intervene early when energy dips
Why Choose AZZ Medical Associates for PDD in New Jersey
Care that fits real schedules: 21+ clinics statewide, HIPAA-secure telehealth, evening options, and same-day appointments. Integrated psychiatry, therapy, and primary care coordination reduces fragmentation. Insurance-friendly access lowers barriers. Local teams know New Jersey’s schools, employers, and communities, so plans match realities, not just ideals, for you.
- 21+ clinics across NJ (same-day visits) and statewide telehealth
- Integrated Psychiatry, therapy, and primary care coordination
- Insurance-friendly: All insurances accepted
- Teen and adult tracks; evening telehealth for commuters and students
- Evidence-based protocols for persistent depressive disorder treatment
Ready to Feel Like Yourself Again?
FAQs
How common is persistent depressive disorder?
How is PDD different from major depression?
PDD is long-term with fewer symptoms; MDD is shorter and more intense. Both can occur together.
Is CBT for persistent depressive disorder available near me in NJ?
Yes. AZZ Medical Associates offers CBT in-clinic at 21+ locations and via HIPAA-secure telehealth near you.
Do medications work for long-term depression disorder?
They can. SSRIs/SNRIs are first-line; adjustments or augmentation are considered if response is partial.
What helps teenagers with persistent depressive disorder?
CBT with parent involvement, school coordination, sleep regularity, and activity scheduling. Telehealth makes access easier during the school year.